
Seminar "Health inequalities in Europe: why so persistent?"
The 15th scientific seminar “Modern Demography” was held on 24 April 2019. The speaker was Johan Mackenbach, MD, PhD, Professor of Public Health, Chair of the Department of Public Health at Erasmus MC, University Medical Center Rotterdam. His report was devoted to health inequalities in Europe, their scope, trends, spatial features and factors determining them. A separate question of the seminar - why the Western European welfare state could not eradicate differences in mortality depending on the socio-economic status of a person?
{kind=link}
{kind=link}
{kind=link}
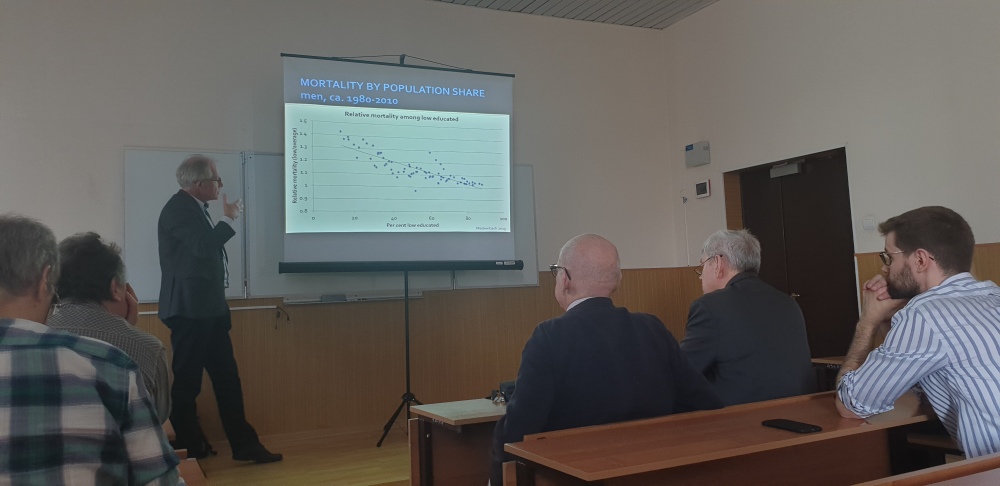
Practically all studies conducted in Europe record significant differences in life expectancy between different educational groups (as a proxy indicator of the socio-economic status of a person) in favor of the “high education” group. If we consider the relative values, i.e. rate ratios the differences in mortality rates (especially from tuberculosis, pneumonia, homicides, lung cancer, and causes caused by alcohol abuse) has increased over time, if we look at the difference in absolute values (rate differences), then these differences have been rather stable. But why did relative differences increase? The answer to this question may lie in the process called “the expansion of education”, which affected all European countries. As a share of the highly educated persons in population grows, the proportion of people with a low level of education decreases, which leads to a stronger negative selection in the latter. At the same time, despite the rapid growth in the share of the highly educated, the positive selection there does not weaken. The possible reasons for this “paradox” are the observed increase in homogeneity of spouses in cohorts by level of education (for men), the growing link between higher education and high income, an increase in the probability for a newborn to be born in a family where at least one of the parents has a higher education.
Differences in behavior (especially concerning health status) between two educational groups are responsible for different health outcomes between them. A typical, but very prominent example is a large gap in the prevalence of smoking (especially large one in Northern and Eastern Europe), which explain a significant part of the differences in mortality between groups of high and low levels of education. In addition, differences in working conditions, in response to stress, and in access to the health care system play a role in the differentiation of mortality by level of education. The factor of poverty (shortage of material wealth), which is much more common among less educated, is also important, especially for Eastern European countries.